Home » Archives for THS Hospital » Page 8
Home » Archives for THS Hospital » Page 8
Home » Archives for THS Hospital » Page 8
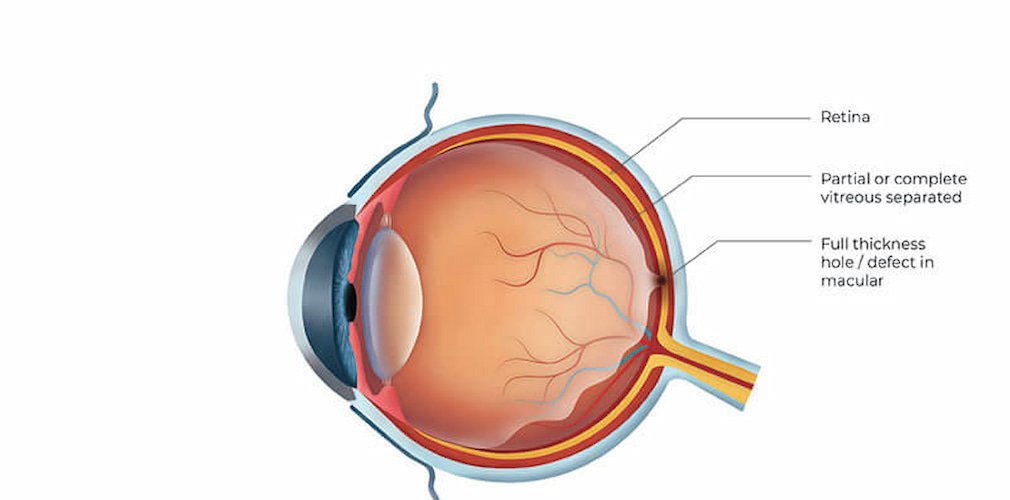
Macular Hole, Epiretinal Membrane & Vitreomacular Traction (VMT)
A
macular hole refers to breakage due to the traction of the center of the retina (macula). The vitreous attached to the retina tractions and in some cases can generate a defect of full thickness, ie a hole in the macula. It is more common in women (3: 1) and can be bilateral (both eyes can be affected) in 15% of cases.
Symptomatology
The clinical manifestations depend on their degree since it is classified in 4 grades. In the beginning, there are no symptoms and, in the last degree (grade 4), there is a significant loss of central vision. If the patient looks at a vertical line of light, he will see that the center is missing.
Exploration
The ophthalmologist when reviewing the fundus will see the macular hole. For its study, OCT (Optical Coherence Tomography) is used as the main method, which will allow establishing the degree of evolution of the patient.
Treatment
The treatment of the macular hole is always surgical. A vitrectomy should be performed with removal of the innermost layer of the retina, called the internal limiting membrane. During the postoperative period, the patient must remain upside down for a few days as gas is placed inside the eye and this position will help to close the hole.
Recently a drug has appeared to inject into the vitreous cavity, which in small cases can release the vitreous traction and close the hole without the need for surgery.
Frequently Asked Questions
Epiretinal membrane with vitreomacular traction is a condition where a thin layer of scar tissue forms on the macula, the central part of the retina, causing distorted or blurred vision. It occurs when the vitreous gel in the eye pulls away from the retina but leaves behind scar tissue that can distort the macula, leading to vision problems.
A macular hole is a small break in the macula, causing central vision loss, while an epiretinal membrane is a thin layer of scar tissue that forms on the macula, leading to distorted or blurred vision. Both conditions affect the macula but present different structural abnormalities and visual symptoms.
VMT, or vitreomacular traction, is a condition where the vitreous gel in the eye remains partially attached to the macula, causing traction and distortion of the central vision.